
nalco group
bone, muscle & joint pain physio
BOOK NOW / WHATSAPP ABOUT YOUR PAIN OR INJURY
- NOVENA 10 Sinaran Drive, Novena Medical Center #10-09, Singapore 307506
- TAMPINES 9 Tampines Grande #01-20 Singapore 528735
- SERANGOON 265 Serangoon Central Drive #04-269 Singapore 550265
Home > Blog > Shoulder Pain Physiotherapy > Shoulder Anatomy
Shoulder Anatomy
 Left shoulder |
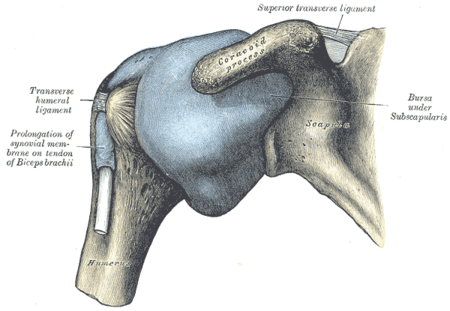 Capsule of shoulder-joint (distended). Anterior aspect. |
Our shoulder joint is one of the most complex joints in our body - it's made up of:
- bones (clavicle aka collar bone; scapula aka shoulder blade; and humerus bone)
- ligaments
- muscles
- tendons
which connects the arm to our torso. There is two shoulder joints that work synergistically and in tandem with each other to allow movement, mobility, strength and function.
shoulder joints
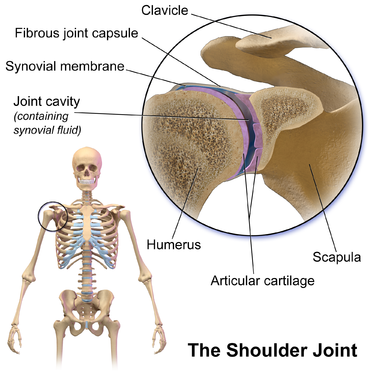
The shoulder joint (also known as the glenohumeral joint) is the main joint of the shoulder. It is a ball and socket joint that allows the arm to rotate in a circular fashion or to hinge out and up away from the body. It is formed by the articulation between the head of the humerus and the lateral scapula (specifically-the glenoid cavity of the scapula).
The "ball" of the joint is the rounded, medial anterior surface of the humerus and the "socket" is formed by the glenoid cavity, the dish-shaped portion of the lateral scapula. The shallowness of the cavity and relatively loose connections between the shoulder and the rest of the body allows the arm to have tremendous mobility, at the expense of being much easier to dislocate than most other joints in the body. There is an approximately 4-to-1 disproportion in size between the large head of the humerus and the shallow glenoid cavity. The glenoid cavity is made deeper by the addition of the fibrocartilaginous ring of the glenoid labrum.
The capsule is a soft tissue envelope that encircles the glenohumeral joint and attaches to the scapula, humerus, and head of the biceps. It is lined by a thin, smooth synovial membrane. This capsule is strengthened by the coracohumeral ligament which attaches the coracoid process of the scapula to the greater tubercle of the humerus. There are also three other ligaments attaching the lesser tubercle of the humerus to lateral scapula and are collectively called the glenohumeral ligaments.
The transverse humeral ligament, which passes from the lesser tubercle to the greater tubercle of humerus, covers the intertubercular groove, in which the long head of biceps brachii travels.
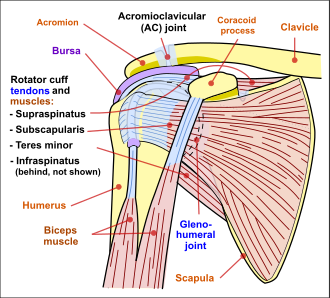
shoulder muscles
 |
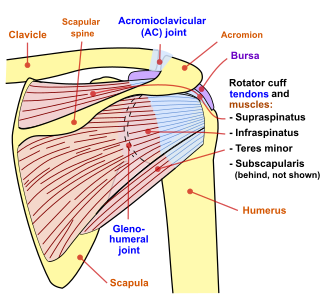 |
The rotator cuff is an anatomical term given to the group of four muscles and their tendons that act to stabilize the shoulder. These muscles are the supraspinatus, infraspinatus, teres minor and subscapularis and that hold the head of the humerus in the glenoid cavity during movement. The cuff adheres to the glenohumeral capsule and attaches to the head of the humerus. Together, these keep the humeral head in the glenoid cavity, preventing upward migration of the humeral head caused by the pull of the deltoid muscle at the beginning of arm elevation. The infraspinatus and the teres minor, along with the anterior fibers of the deltoid muscle, are responsible for external rotation of the arm.
The four tendons of these muscles converge to form the rotator cuff tendon. This tendon, along with the articular capsule, the coracohumeral ligament, and the glenohumeral ligament complex, blend into a confluent sheet before insertion into the humeral tuberosities. The infraspinatus and teres minor fuse near their musculotendinous junctions, while the supraspinatus and subscapularis tendons join as a sheath that surrounds the biceps tendon at the entrance of the bicipital groove.
shoulder function
The muscles and joints of the shoulder allow it to move through a remarkable range of motion, making it one of the most mobile joints in the human body. The shoulder can abduct, adduct, rotate, be raised in front of and behind the torso and move through a full 360° in the sagittal plane.
This tremendous range of motion also makes the shoulder extremely unstable, far more prone to dislocation and injury than other joints.
Clinical significance
The shoulder is the most movable joint in the body. However, it is an unstable joint because of the range of motion allowed. This instability increases the likelihood of joint injury, which often leads to a degenerative process in which tissues break down and no longer function well.[citation needed]
Fracture
Fractures of shoulder bones can include clavicular fractures, scapular fractures, and fractures of the upper humerus.
Pain
Shoulder problems, including pain, are common and can relate to any of the structures within the shoulder. The primary cause of shoulder pain is a rotator cuff tear. The supraspinatus is most commonly involved in a rotator cuff tear.[citation needed]
When this type of cartilage starts to wear out (a process called arthritis), the joint becomes painful and stiff.
- Arthritis
- Frozen shoulder
- Impingement syndrome
- Shoulder dislocation
Shoulder imaging
Imaging of the shoulder includes ultrasound, X-ray and MRI, and is guided by the suspected diagnosis and presenting symptoms.
Conventional x-rays and ultrasonography are the primary tools used to confirm a diagnosis of injuries sustained to the rotator cuff. For extended clinical questions, imaging through Magnetic Resonance with or without intraarticular contrast agent is indicated.
Hodler et al. recommend starting scanning with conventional x-rays taken from at least two planes, since this method gives a wide first impression and even has the chance of exposing any frequent shoulder pathologies, i.e., decompensated rotator cuff tears, tendinitis calcarea, dislocations, fractures, usures, and/or osteophytes. Furthermore, x-rays are required for the planning of an optimal CT or MR image.
The conventional invasive arthrography is nowadays being replaced by the non-invasive MRI and ultrasound, and is used as an imaging reserve for patients who are contraindicated for MRI, for example pacemaker-carriers with an unclear and unsure ultrasonography.
X-ray
Projectional radiography views of the shoulder include:
AP-projection 40° posterior oblique after Grashey
The body has to be rotated about 30 to 45 degrees towards the shoulder to be imaged, and the standing or sitting patient lets the arm hang. This method reveals the joint gap and the vertical alignment towards the socket.[21]
Transaxillary projection
The arm should be abducted 80 to 100 degrees. This method reveals:
- The horizontal alignment of the humerus head in respect to the socket and the lateral clavicle in respect to the acromion
- Lesions of the anterior and posterior socket border, or of the tuberculum minus
- The eventual non-closure of the acromial apophysis
- The coraco-humeral interval
Y-projection
The lateral contour of the shoulder should be positioned in front of the film in a way that the longitudinal axis of the scapula continues parallel to the path of the rays. This method reveals:
- The horizontal centralization of the humerus head and socket
- The osseous margins of the coraco-acromial arch and hence the supraspinatus outlet canal
- The shape of the acromion
This projection has a low tolerance for errors and, accordingly, needs proper execution. The Y-projection can be traced back to Wijnblath’s 1933 published cavitas-en-face projection.
BOOK NOW / WHATSAPP ABOUT YOUR PAIN OR INJURY
- NOVENA 10 Sinaran Drive, Novena Medical Center #10-09, Singapore 307506
- TAMPINES 9 Tampines Grande #01-20 Singapore 528735
- SERANGOON 265 Serangoon Central Drive #04-269 Singapore 550265
where to next?
- Book an appointment here.
- See our Shop / products page to search for possible solutions that may help your aches, pain and injuries =)
- Sign up to be a NALCO Insider (newsletter), and get special treatment such as deals, promotions and be the first to find out developments from the inside =)
- Read up on your possible pain injuries and causes at the Conditions section.
- First time coming to our physio & hand therapy clinic?
a) Check out the Frequently Asked Questions (FAQ).
b) See our Singapore physio and hand therapy clinic locations and how to get to us
c) Can you claim for your physio or hand therapy sessions? Read more here. - Take a look at the case studies and patient testimonials we'd gotten since 2006.
- Find Orthopedic Doctors in Singapore We Trust and Recommend for first, second or even third opinions, whom we know professionally and had work with for years...and whom we'd also trust our families with.
- Contact us on any pains or injuries that you're unsure of, or if you're in Singapore and want physiotherapy or hand therapy treatment for pains and injuries.
- Go back to NalcoGroup Home page
Disclaimer: NalcoGroup.com publishes content around painful conditions or injuries of the bone, muscle and joint but they are NOT medical advice. Consult your regular doctor. Affiliate disclaimer: there are some products by which if you buy through our links, we may be paid a small affiliate commission for. These are not paid sponsorship and we are not paid to list them - most of the products we recommend through our sites are either personally tested by ourselves or are something we already use in our clinic practice. We do not endorse any specific products - purchase them at your own discretion.